Transcription of Chapter 13 and Resections Axillary Space Exploration
1 1 Axillary Space Exploration and ResectionsChapter13 James C. Wittig, Martin M. Malawer, Kristen Kellar-Graney,and Robert M. HenshawBACKGROUND The axilla is a common site for primary soft tissue sarco-mas as well as for metastatic disease that involves the axillarylymph nodes, such as advanced breast cancer or melanoma. Sarcomas typically arise from the muscles defining the axil-lary Space (FIG 1). Occasionally, however, they may arise di-rectly from the brachial plexus or Axillary vessels (eg, malig-nant peripheral nerve sheath tumors, neurosarcoma,leiomyosarcoma). Several types of malignant tumors may in-volve the Axillary Space and may require surgical sarcomas occur within the muscles (ie, the pectoralismajor, latissimus dorsi, teres major, and subscapularis mus-cles) that make up the borders of the Axillary Space . Rarely dothey develop within the Axillary fat itself. More commonly,large metastatic deposits to the regional lymph nodes createlarge, matted masses that may require resection.
2 The mostcommon of these are metastatic melanoma and recurrentbreast carcinoma. In addition, there are primary tumors thatarise from the brachial plexus, either the nerves or the include leiomyosarcomas of the Axillary vein and neu-rofibrosarcomas of the adjacent nerves. Small masses may be clinically silent, but large masses in-evitably will result in significant pain or loss of function due toinvolvement of the brachial plexus. Venous occlusion may be seen in neglected, massive tumorsand is a harbinger of loss of limb and possibly even of life dueto gangrene. Historically, surgical management of tumors in this locationconsisted of forequarter amputation; advances in radiographicimaging, adjuvant therapies, and surgical techniques havegreatly improved our ability to perform limb-sparing resec-tions in this location. The key to adequate and safe surgical re-section of Axillary tumors is the complete visualization andmobilization of the infraclavicular portion of the brachialplexus and the Axillary artery and vein and the cords that sur-round them.
3 In general, imaging studies of the Axillary spaceare not reliable for determining vascular or nerve sheath in-volvement. Multiple imaging studies are required, but the ulti-mate decision to proceed with a limb-sparing surgery is basedon the intraoperative findings at the time of Exploration . Axillary tumors extending along the chest wall often can beelevated off the underlying ribs; however, tumor extensioninto the intercostal spaces may require thoracotomy and ribresection to ensure adequate The axilla is a pyramid-shaped Space between the chest walland the arm defined by its surrounding muscles; it appears tri-angular when seen from either the coronal or axial views. The superior apex of the pyramid is formed by the junctionof the clavicle and the first rib, approximately 1 to 2 cm me-dial to the coracoid process. The muscular boundaries of the axilla consist of the pectoralismajor muscle anteriorly; the subscapularis, teres major, andlatissimus dorsi muscles posteriorly; and the coracobrachialis,short head of the biceps, and triceps muscles laterally.
4 Vital structures in the axilla include the major branches ofthe infraclavicular portion of the brachial plexus and the axil-lary vessels. Any surgery in this region requires detailedknowledge of and familiarity with these structures. Infraclavicular brachial plexus The lateral, posterior, and medial cords of the infraclavic-ular brachial plexus are found at the level of the pectoralisminor muscle, where they then give rise to five majorbranches: the median, ulnar, radial, musculocutaneous, andaxillary nerves. The cords and branches run along the axil-lary vascular sheath as it passes through the axilla. The lateral cord gives rise to the musculocutaneous nerve,which travels along the medial aspect of the conjoint ten-don, where it innervates the coracobrachialis and short headof the biceps. This nerve is the first to be identified duringthe Exploration , because it is located in the superficial axil-lary fat inferior to the coracoid process. The largest portionof the lateral cord combines with the medial cord to createthe median nerve.
5 The posterior cord gives rise to the Axillary nerve, whichtravels deep in the Space and passes inferior to the gleno-humeral joint and subscapularis muscle, where it innervatesthe deltoid muscle. The main portion of the posterior cordbecomes the radial nerve, which travels posterior to thesheath and exits the Axillary Space along with the axillarysheath. The medial cord gives rise to the ulnar nerve, which trav-els along the most medial aspect of the sheath and exits dis-tally along with the sheath. Because of its medial positionalong the sheath, the ulnar nerve is the nerve most com-monly involved by tumors arising inferior to the brachialplexus, which can present with symptoms of either weak-ness or neuropathic pain. The median nerve, formed by acombination of the lateral and medial cords, is found on thelateral aspect of the sheath and exits the inferior aspect ofthe Axillary Space along the sheath.
6 Axillary vessels The Axillary artery and vein are the continuation of thesubclavian vessels, changing name as they enter the apex ofthe axilla below the clavicle and first rib. These vessels runin a single sheath, surrounded by the cords of the brachialplexus. The vessels pass through the Axillary Space medial tothe coracoid to the medial aspect along the humeral to the teres major, the vessels are renamed thebrachial vascular branches in the axillaryspace include the thoracoacromial artery (with its pectoral,deltoid, clavicular and acromial branches), the lateral tho-racic artery, the subscapular artery, and the anterior andposterior humeral circumflex 3/22/09 9:58 AM Page 12 Part 4 ONCOLOGY Section IISHOULDER GIRDLE AND UPPER EXTREMITIES Lymphatics A substantial amount of fat surrounds the vascular sheathas it runs through the axilla along with the lymphatics andlymph nodes. Major clusters of lymph nodes are foundalong the brachial and Axillary vessels, the lateral thoracicvessels (anterior Axillary nodes), and the subscapular vessels(posterior Axillary nodes).
7 Axillary tumors may arise fromlymph node metastases anywhere along the Axillary vessels;the most common sites are nodes along the distal portion ofthe Axillary Any mass in the Axillary Space should be considered forbiopsy or resection given the propensity for malignant tumorsto develop in the axilla and the predictability of neurogenicpain arising from continued tumor growth. Palpate radial and ulnar pulses and inspect for venouscongestion or swelling. Consider venography to evaluate lossof venous drainage indicative of tumor involving the brachialplexus. Dimunition of arterial flow is a late sign indicative of poten-tial loss of limb consider forequarter amputation. Test sensation and strength of the Axillary , radial, median,and ulnar nerves. Loss of nerve function typically is a very latefinding indicative of major tumor involvement of the brachialplexus consider forequarter amputationIMAGING AND OTHER STAGINGSTUDIES Three-dimensional imaging of the Axillary Space is impor-tant for accurate anatomic tumor localization and surgicalplanning.
8 CT, MRI, angiography, and three-phase bone scansare used in the same manner as in other anatomic sites. In ad-dition, we have found that venography (of the Axillary andbrachial veins) is essential to the evaluation of tumors of theaxilla and brachial Radiography Careful inspection of posterior anterior chest, anterior shoul-der, and Axillary view radiographs may reveal the presence of -increased soft tissue density corresponding to an Axillary mass. Bone involvement and the presence of calcifications in thesoft tissues should be Tomography and Magnetic ResonanceImaging Multiplanar MRI is extremely helpful in visualizing theanatomic contents of the Axillary Space and defining theanatomic extent of the tumor (FIG 2A C). Axial CT imaging, with administration of IV contrast,demonstrates the major vascular structures, outlines the majormuscle planes, and can detect subtle matrix formation withinthe tumor. CT is most useful in evaluating the bony walls ofthe axilla, specifically the humerus, glenohumeral joint, andscapula (FIG 2D).
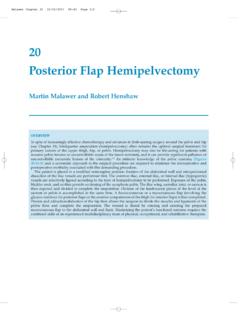
9 Certain tumors, such as lipomas or hemangiomas, may havecharacteristic findings on T1- and T2-weighted MRI sequencessuggestive of the proper histologic diagnosis. The presence orabsence of lymphatic involvement should be noted, particu-larly in patients with a history of metastatic carcinoma. Although the brachial plexus may be very difficult to visual-ize, particularly when tumors distort or compress the sur-rounding fatty planes, the anatomic relationship of the nervesheath to the vessels helps pinpoint their location. Although CT imaging of the lungs is routinely performed aspart of patient staging, the chest wall should always be in-spected carefully to rule out tumor involvement of the rib cageand pleural Imaging Positron emission tomography (PET) imaging, particularlywhen fused with MRI or CT imaging data, may significantlyimprove the ability to detect lymphatic spread of tumor in andaround the axilla. Standardized uptake values (SUV) correlateABFIG 1 Anatomy of the Axillary Space .
10 Of the shoulder girdle and axilla showing the bony andsoft tissue contents. The Axillary artery enters from the clavicle and exits at the lower portion of the axilla atthe level of the pectoralis major and latissimus dorsi muscles. The overlying pectoralis major muscle formingthe anterior wall and the latissimus dorsi muscle forming the posterior wall is visualized. scan of anormal axilla. All of the muscles of the anterior and posterior wall as well as the deltoid are 3/22/09 9:58 AM Page 2 Chapter 13 Axillary Space Exploration AND RESECTIONS3with tumor metabolism and may help to distinguish betweenbenign and malignant and Other Studies Angiography remains a valuable method of imaging the ax-illa, particularly for preoperative planning, because tumorsmay significantly distort the regional vascular anatomythrough mass effect as well as through angiogenesis (ie, forma-tion of abnormal vessels feeding the tumor; FIG 3).Venography, either alone or in conjunction with angiography,can demonstrate venous compression from surrounding tu-mors.