Transcription of Use of Allografts and Chapter 29 Reconstruction of ...
1 1 BACKGROUND An intercalary Reconstruction is defined as replacement ofthe diaphyseal portion of a long bone after segmental skeletalresection (diaphysectomy). Intercalary reconstructions typically result in superior func-tion compared to other limb-sparing procedures because thepatient s own joints above and below the Reconstruction areleft undisturbed. Most intercalary reconstructions are performed with bulkallografts, although various endoprosthetic intercalary pros-theses are available. Allograft reconstructions require osseous healing for long-term stability; initial allograft stability must be obtained withintramedullary nailing or internal fixation. Allografts have a long-term risk of fracture likely related tothe size and type of fixation. Intercalary Allografts are often supplemented with vascular-ized fibular grafts. Endoprosthetic Reconstruction has typically been limited tosmall, central tumors as significant lengths of bone proximaland distal to the lesion are required for successful fixation oftraditional prosthetic stems.
2 New implant designs have expanded the indication for inter-calary prostheses by drastically reducing the length of boneneeded to achieve stable fixation. Segmental prostheses typically provide immediate stable fixa-tion, allowing early rehabilitation and rapid return of function. Vascularized fibular grafts are not required for intercalaryimplants. Although aseptic loosening has been reported after endo-prosthetic Reconstruction , it is rarely if ever seen with inter-calary implants; the lack of bearing surfaces contributing towear debris formation and the lack of exposure to joint fluidhelp to protect the Intercalary reconstructions are indicated for osseous joint-sparing reconstructions. Intercalary reconstructions are performed most commonlyin the femur, tibia, humerus, and forearm. Intercalary reconstructions require adequate remainingbone stock to allow stable fixation; if inadequate bone re-mains, the procedure should be converted to a joint-replacingreconstruction.
3 Intercalary allograft reconstructions require osseous heal-ing for long-term stability, which can be compromised bychemotherapy or radiation during the healing period. Intercalary Allografts in areas with poor vascularity, withsmall residual host segments, in heavy or very active patients,or with planned radiation or chemotherapy likely benefit fromsupplemental vascularized fibular Allografts . Intercalary endoprosthetic Reconstruction is an option ifallograft Reconstruction is contraindicated due to poor hostfactors or in patients with prior failed allograft Reconstruction . Modular intercalary prostheses provide the flexibility toeasily convert to a conventional endoprosthetic replacement ei-ther at initial surgery or for later revisions by using joint-replac-ing modules at either end of the Anatomic considerations in the femur include the anteriorbow, femoral anteversion, and the proximity of the superficialfemoral artery to the distal femur near the adductor hiatus.
4 Anatomic considerations in the tibia include the limited softtissue coverage anteromedially and the proximity of the poste-rior tibial neurovascular bundle to the posteromedial tibia. Anatomic considerations in the humerus include the prox-imity of the radial nerve to the posterior midhumeral shaft. Anatomic considerations in the forearm include the HISTORY AND PHYSICAL FINDINGS Table 1 outlines methods for examining the patient with amass or suspected tumor. Important aspects of the patient history include: Onset of mass or pain Progression of growth or pain Constitutional symptoms (fevers, chills, night sweats,weight loss) Personal or family history of cancerIMAGING AND OTHER STAGING STUDIES Radiographs are the primary imaging study used in forminga differential diagnosis of bone lesions. Radiographs are used to assess the geometry and size of thehost bone and the lesion to allow appropriate sizing of the al-lograft Reconstruction .
5 Radiographs are helpful in determining the response tochemotherapy, which influences the decision making for limbsalvage. Bone scan is used to determine if there are additional os-seous sites of disease. Computed tomography (CT) scanning is used to determine thebone geometry and to assess bone destruction by a lytic lesion. Magnetic resonance imaging (MRI) is used to assess the softtissue extension of a lesion. It is also used to assess the prox-Chapter29 Walter W. Virkus, Robert M. Henshaw, Benjamin Miller, and Steven GitelisUse of Allografts andSegmental Prostheses forReconstruction of SegmentalBone 5/13/09 9:13 AM Page 1imity of neurologic and vascular structures, the intraosseous ormarrow extent of tumor, and extension into an adjacent joint. Sagittal and coronal MRI images are extremely useful in plan-ning the resection length; measurements from the adjacent jointsto the planned levels of osteotomy are made to provide a repro-ducible method of identifying the levels intraoperatively.
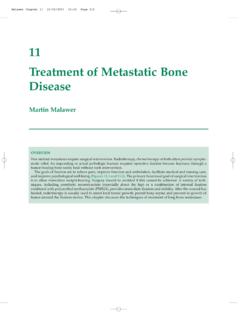
6 The role of positron emission tomography (PET) scanninghas yet to be defined for sarcomas. It likely plays a role in theassessment of metastatic MANAGEMENT The main surgical decisions to be made when performing anintercalary resection are the type and length of fixation and theneed for supplemental vascularized fibula graft. Plate fixation allows for Reconstruction with standard os-teosynthesis techniques. Plate fixation allows for compression across the allograft hostjunctions, which likely improves healing. Plate fixation results in screw holes in the allograft, which isthought to contribute to late allograft fracture. Intramedullary fixation of Allografts requires additional in-cisions but likely provides stronger fixation. Intramedullary fixation provides long-term protection of theallograft without placing screw holes in the allograft (FIG 1). Intramedullary fixation makes it difficult to obtain compres-sion at the allograft host junctions, which may impede healing.
7 Allograft and host cuts can be transverse or stepped (FIG 2). Transverse cuts make rotational adjustments easier and likelyresult in less periosteal dissection, which may improve healing. Stepped cuts are more technically difficult, add surgical time,and may cause more damage to the local periosteum. However,they likely increase host allograft bone contact, which may im-prove healing. Intercalary implants require careful attention to resectionlength and canal preparation to ensure optimal fixation of theimplant stems. Regardless of the method of skeletal Reconstruction , carefulattention to the soft tissues and use of rotational muscle flapswhen indicated are necessary to reduce the risk of wound com-plications and subsequent Planning Preoperative planning is extraordinarily critical in thesecomplex reconstructive procedures. Multiple imaging techniques should be used to fully assess thetumor, length of resection, and the remaining bone anatomynecessary to support the planned Reconstruction .
8 Standard instruments for tumor resection are required, in-cluding bone saws; equipment for additional procedures suchas vascular bypass, vascularized graft, or specialized soft tissuereconstruction should be available. Some surgeons prefer to use a separate group of instrumentsfor the resection and the the borders of the mass to evaluate size and whether Lack of mobility suggests adherence to surrounding is mobile from the surrounding range of motionAssess range of motion of joints adjacent to masses may restrict joint tissue evaluationAssess soft around mass or biopsy to determine resectionAlternative methods of wound closure may be required at approach and whether sufficient soft tissue remains to the time of primary examinationAssess circulation of compromise may complicate limb 1 Methods for Examining the Patient with a Mass or Suspected TumorABFIG 1 Placement of intramedullary nail and compressionof junction.
9 View of intramedullary nailthrough allograft in the proximal femur. The K-wire forrotational reference can be seen. Gaps in the host graftjunction are present without compression of the view after placement and tightening of com-pression screw in intramedullary nail. Gap at host allograftjunction is 4 ONCOLOGY Section IVLOWER 5/13/09 9:13 AM Page 2 Chapter 29 Allografts AND SEGMENTAL PROSTHESES FOR Reconstruction OF SEGMENTAL BONE DEFECTS3 The allograft needs to be ordered from a bone bank. Somesurgeons prefer to size-match Allografts used for intercalary re-constructions, requiring radiographs of the allograft to be ob-tained before ordering. If a vascularized fibula graft is planned, the timing and hostlocation of the graft must be determined. Endoprosthetic implants may require customized compo-nents, typically requiring a 3- to 4-week lead time to allow fordesign and manufacturing of the implant. An examination under anesthesia focusing on the rotationalprofile of the nonoperative leg can be useful in ensuring properrotation of the operative leg.
10 Intraoperative C-arm fluoroscopy is useful to measure andselect the levels of planned bone Positioning depends on the tumor location and the surgicalapproach required for oncologic resection. Femoral resections are typically performed either in thesupine or lateral position; tibial cases are performed supine. Femoral reconstructions may be facilitated by a bump underthe buttock, but this may make clinical assessment of rotationmore difficult. Forearm reconstructions are performed with the patientsupine and the arm on a hand table. Humeral reconstructions can be performed with the patientin the supine or beach chair The approach for intercalary reconstructions is determinedby the incision needed to perform an adequate resection of thetumor. Femoral reconstructions are ideally performed through alateral or anterolateral approach to the thigh; medial incisionsmay be necessary to isolate and protect the superficial femoralartery and vein during the resection.