Transcription of Echocardiography in aortic diseases: EAE recommendations ...
1 RECOMMENDATIONSE chocardiography in aortic diseases: EAE recommendations for clinical practiceArturo Evangelista1*, Frank A. Flachskampf2, Raimund Erbel3,Francesco Antonini-Canterin4, Charalambos Vlachopoulos5, Guido Rocchi6,Rosa Sicari7, Petros Nihoyannopoulos8, and Jose Zamorano9on behalf of theEuropean Association of EchocardiographyDocument Reviewers: Mauro Pepia, Ole-A. Breithardtb, and Edyta Plon ska-Gos ciniakc1 Servei de Cardiologia, Hospital Vall d Hebron, P8 Vall d Hebron 119, 08035 Barcelona, Spain;2 University of Erlangen, Erlangen, Germany;3 University of Essen, Essen, Germany;4 Hospital Pordenone, Pordenone, Italy;5 Hippokration Hospital, Athens, Greece;6S. Orsola University Hospital, Bologna, Italy;7 Institute of Clinical Physiology, Pisa, Italy;8 Hammersmith Hospital, London, UK; and9 Hospital Cl nico San Carlos, Madrid, SpainaInstituto di Cardiologia dell Universita`degli Studi. Milan, Italy;bMedizinische Klinik 2, University Hospital, Erlangen, Germany; andcPomeranian Medical School, Szczecin, PolandReceived 28 March 2010; accepted after revision 29 March 2010 Echocardiography plays an important role in the diagnosis and follow-up of aortic diseases.
2 Evaluation of the aorta is a routine part of thestandard echocardiographic examination. Transthoracic Echocardiography (TTE) permits adequate assessment of several aortic segments,particularly the aortic root and proximal ascending aorta . Transoesophageal Echocardiography (TOE) overcomes the limitations of TTEin thoracic aorta assessment. TTE and TOE should be used in a complementary manner. Echocardiography is useful for assessing aorticsize, biophysical properties, and atherosclerotic involvement of the thoracic aorta . Although TOE is the technique of choice in the diagnosisof aortic dissection, TTE may be used as the initial modality in the emergency setting. Intimal flap in proximal ascending aorta , pericardialeffusion/tamponade, and left ventricular function can be easily visualized by TTE. However, a negative TTE does not rule out aortic dissectionand other imaging techniques must be considered. TOE should define entry tear location, mechanisms and severity of aortic regurgitation,and true lumen compression.
3 In addition, Echocardiography is essential in selecting and monitoring surgical and endovascular treatment andin detecting possible complications. Although other imaging techniques such as computed tomography and magnetic resonance have agreater field of view and may yield complementary information, Echocardiography is portable, rapid, accurate, and cost-effective in the diag-nosis and follow-up of most aortic diseases Transoesophageal Echocardiography Transthoracic Echocardiography ContrastechocardiographyIntroductionAort ic diseases are an important cause of cardiovascular morbidityand mortality. Except when complications are life-threatening, suchas acute aortic syndrome or aortic rupture, aortic diseases areasymptomatic and without abnormalities on physical examination;thus, diagnosis and follow-up depend exclusively on imaging tech-niques. Echocardiography has become the most used imaging testin the evaluation of cardiovascular disease and plays an importantrole in the diagnosis and follow-up of aortic diseases.
4 The aorta isdivided into segments: the aortic root, ascending aorta , aortic arch,descending aorta , and abdominal aorta . Ultrasound techniques forimaging of the aorta include transthoracic Echocardiography (TTE),transoesophageal Echocardiography (TOE), abdominal ultrasound,and intravascular ultrasound (IVUS). In the present article, we willfocus on TTE and TOE methodologies in the assessment of aorticdiseases, their strengths and limitations for its use in various clinicalsituations and recommendations for appropriate applications of*Corresponding author. Tel:+34 932746212; fax:+34 932746244, Email: on behalf of the European Society of Cardiology. All rights Author 2010. For permissions please email: Journal of Echocardiography (2010)11, 645 658 by guest on January 17, from Echocardiography based on available evidence. It is not the mainobjective of this manuscript to compare the usefulness of echocar-diography with other imaging techniques or to describe the stan-dard diagnostic management of different aortic echocardiographyEchocardiographic evaluation of the aorta is a routine part of thestandard echocardiographic TTE is notthe technique of choice for overall assessment of the aorta , it isuseful for the diagnosis and follow-up of some segments of theaorta.
5 TTE is one of the techniques most used to measure proxi-mal aortic segments in clinical practice. Using different windows,the proximal ascending aorta is visualized in the left and right para-sternal long-axis views (Figure1) and, to a lesser extent, in basalshort-axis views. The long-axis view affords the best opportunityfor measuring aortic root diameters by taking advantage of thesuperior axial image resolution. In all patients with suspectedaortic disease , the right parasternal view is recommended for esti-mating the true size of the ascending aorta . The ascending aorta isalso visualized in the apical long-axis and modified apical five-chamber views; however, in these views, the aortic walls areseen with suboptimal lateral resolution. Modified subcostal viewsmay in some cases (more frequently in children) be helpful, buthere the ascending aorta is far from the transducer.
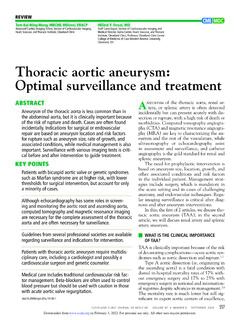
6 All theseviews also permit assessment of the aortic valve, which is ofteninvolved in diseases of the ascending aorta ( bicuspid valve, aortic regurgitation due to dilatation of the ascending aorta oraortic dissection, and other diseases).Of paramount importance for evaluation of the thoracic aorta isthe suprasternal view (Figure2A). This view primarily depicts theaortic arch and the three major supra- aortic vessels (innominate,left carotid, and left subclavian arteries), with variable lengths ofthe descending and, to a lesser degree, ascending aorta . AlthoughFigure 1 Transthoracic Echocardiography . (A) Parasternallong-axis view (transthoracic Echocardiography ). The followingdiameters are shown: outflow tract diameter (1), sinuses of Val-salva (2), sinotubular junction (3), and tubular ascending aorta (4).(B) Right parasternal long-axis view, mid and distal parts ofascending aorta may be visualized.
7 AAo, ascending aorta ; LA,left atrium; LV, left ventricle; RV, right 2(A) Suprasternal view of aortic arch and supra- aortic great arteries. (B) Mid part of the descending thoracic aorta visualized by long-axis view from apical window. (C) Abdominal aorta visualized by subcostal view. In non-obese patients, it is not difficult to visualize distalabdominal aorta . art, artery; PA, pulmonary artery; AAo, ascending aorta ; DAo, descending aorta ; CT, coeliac Evangelistaet by guest on January 17, from this view may be obstructed, particularly in patients with emphy-sema or short, wide necks, it should be systematically sought ifaortic disease is evaluated. From this window, aortic coarctationcan be visualized and functionally evaluated by continuous-waveDoppler; a persistent ductus arteriosus may also be identifiableby colour Doppler. Dilatation and aneurysm, plaque, calcification,thrombus, or a dissection membrane are detectable if imagequality is sufficient.
8 A systematic comparison of harmonic TTEand TOE made to detect aortic plaques and thrombi revealedhigh sensitivity for the detection of aortic arch atheromas protrud-ing 4 mm into the entire thoracic descending aorta is not well visualized byTTE. A short-axis view of the descending aorta can be imaged pos-teriorly to the left atrium in the parasternal long-axis view. Fromthe apical window, a short-axis cross-section of the descendingaorta is seen lateral to the left atrium in the four-chamber viewand a long-axis stretch in the two-chamber view. By 908transdu-cer, a rotation long-axis view is obtained and a mid part of the des-cending thoracic aorta may be visualized (Figure2B). Although apartial assessment of the size of the descending aorta and detec-tion of large abnormal structures such as dissection membranesare possible in these views, the descending aorta lies far fromthe transducer and the assessment is incomplete, suboptimal andnot accurate.
9 However, in acute aortic syndrome with leftpleural effusion, scanning from the back may provide good oroptimal views of the descending contrast, since the abdominal descending aorta is relativelyeasily visualized to the left of the inferior vena cava in sagittal(superior inferior) subcostal views, the systematic search forabdominal aortic aneurysms has been advocated as part of theroutine echocardiographic exam3,4(Figure2C), although transthor-acic echo transducers are not optimal for abdominal summary, although TTE is not the ideal tool for visualizing allaortic segments, important information can always be gained bycareful use of all echo windows (Table1)..Table 1 Echocardiographic views of the aortaViewPart of aortaTransthoracic echoParasternal long+short axisAscending+descending thoracicApical four-chamberDescending thoracicApical two-chamber and/orlong axisDescending thoracicSuprasternalArch, descending+ascendingthoracicSubcostalAbd ominal (+ascending thoracic)Transoesophageal echoUpper oesophageallong+short axisAscending thoracicAortic (long+short axis)Descending thoracic+archFigure 3 Transoesophageal Echocardiography .
10 (A) Ascending aorta in long-axis view at 1208.(B) aortic arch in transverse view. (C) Descend-ing aorta visualized by transverse view. (D) Descending aorta visualized by longitudinal in aortic diseases647 by guest on January 17, from RecommendationTTE permits adequate assessment of several aortic segments, par-ticularly the aortic root and proximal ascending aorta . All scanningplanes should be used to obtain information on most aortic seg-ments. However, if inconclusive information or abnormalities arepresent, another imaging modality is required to either completeor add diagnostic of the oesophagus and the thoracic aorta permits high-resolution images from higher-frequency TOE. Furthermore, theavailability of multiplane imaging permits improved incrementalassessment of the aorta from its root to the descending most important transoesophageal views of the ascendingaorta, aortic root and aortic valve are the high transoesophageallong-axis (at 1208 1508)(Figure3A) and short-axis (at 308 608)views.