Transcription of Paediatric Clinical Practice Guideline
1 Paediatric Clinical Practice Guideline Paediatric Clinical Practice Guideline Hypertension Page 1 of 8 Hypertension Author: Dr P Hildick-Smith, Dr M Lazner, Mr C Chadwick Approved by the Medicines Governance Group October 2019 Publication date: October 2019 Review date: October 2021 Definitions (all on the basis of age, sex and height tables): In children with known renal problems the blood pressure should be maintained around the 50th percentile. Assessment Measurement of Blood Pressure in Children - Use the right side upper arm - Use a cuff that is appropriate to the size of the child s arm. If a cuff is too small, the next largest cuff should be used, even if it appears large. Bladder length should be 80 100% of the upper arm circumference Bladder width should be at least 40% of the upper arm length - Manual measurements will always be more accurate than machine measurements.
2 If the initial BP is elevated ( 90th percentile), it is most likely to be artificially elevated due to anxiety. It is therefore important to get serial measurements for a more accurate picture. Perform 2 additional BP measurements at the same visit and average them. Ensure a manual measurement has been obtained. Check cuff size is correct. Child needs to be calm if upset will get a high reading which cannot be interpreted. Blood Pressure Tables See Appendices 1 (boys) and 2 (girls) NB. Use a height chart to determine the height percentile. Also, ensure you use the correct gender table for blood pressure Click here for an online version. Normal blood pressure (BP) = average systolic and/or diastolic blood pressure (SBP/DBP) <90th percentile or < 120/<80 mmHg in adolescents Elevated BP = SBP and/or DBP 90th percentile and <95th percentile; or for adolescents, BP 120/80 mm Hg to <95th percentile, or 90th and <95th percentile, whichever is lower.
3 Hypertension = average clinic measured SBP and/or DBP 95th percentile on three or more occasions. Paediatric Clinical Practice Guideline Paediatric Clinical Practice Guideline Hypertension Page 2 of 8 Diagnostic evaluation History / examination / investigations Essential or primary hypertension is a diagnosis of exclusion in children. Aims of investigations are to determine an underlying cause and establish whether there is evidence of end organ damage. Renal disease is the commonest cause of secondary hypertension in children. Record FH of hypertension or renal problems / child s diet and activity / drug history. Record weight, height and BMI. Always consider an undiagnosed coarctation of the aorta - feel for femoral pulses and perform BP in upper and lower limbs.
4 BP usually 10-20 mmHg higher in legs than arms, in coarctation this is reversed. Initial screening investigations: Second line investigations: Complement & auto-antibody screen Plasma renin, aldosterone ACTH, free cortisol Thyroid function tests Urinary catecholamines MR/CT angiography Renal angiography and renal vein renin studies** MIBG scan** **Only done in tertiary care What to do when BP is raised in CED, the wards or general Paediatric clinic setting 1. If BP normal or normalises after repeat measurement: No further action required. Repeat BP at next health care encounter. 2. If BP elevated (BP 90th percentile but < 95th percentile) Patient needs serial measurements over the next 4 6 weeks.
5 This can be done by GP Practice weekly, or, using a home monitor with a properly sized cuff, or, community nurses. BP persistently high 90th percentile < 95th percentile Check upper and lower limb BP (right arm, left arm and left leg) Refer to Paediatric outpatient clinic Consider initiating first line investigations as over Blood: FBC, U&Es, lipid profile Urine dipstick & microscopy Urine protein: creatinine ratio Renal ultrasound with doppler ECG Echo Paediatric Clinical Practice Guideline Paediatric Clinical Practice Guideline Hypertension Page 3 of 8 3. If hypertension present (BP 95th percentile) Ambulatory Blood Pressure Measurement (ABPM) Will be done in clinic setting if required, refer to Paediatric outpatient clinic Useful to rule out reactive raised blood pressure seen when a child is anxious.
6 Also decreases the chance of over diagnosis of raised BP. Allows evaluation of hypertension, particularly readings overnight. Absence of a normal nocturnal dip is associated with poorer outcomes and those at risk for end organ damage. Can also be used to evaluate response to drug treatment. Treatment The aim of treatment is to bring the blood pressure between the 50th & 75th percentile for height & gender. Specific treatment depends on the cause, duration and severity of the hypertension. Treatment options should be discussed with the Paediatric Renal Team. If pharmacological therapy is to be initiated on the advice of the Consultant, please contact a member of the Pharmacy team to discuss suitable formulation and arrangements for supply.
7 Notes: When to Measure Blood Pressure All healthy children 3 years who are seen in a medical setting should have their BP measured at least once per year. The following children 3 years should have their BP measured at every health encounter: Obesity Diabetes Treatment with drugs known to raise BP Congenital heart disease, especially aortic arch obstruction or coarctation Known renal disease Ambulatory BP measurement with urgent OP review (< 2 weeks) or frequent BP measurements as in-patient d/w CED consultant or COW Start diagnostic evaluation Consider referral to cardiology / renal team at ECH Paediatric Clinical Practice Guideline Paediatric Clinical Practice Guideline Hypertension Page 4 of 8 Children < 3 years with the following should have their BP measured.
8 History of prematurity or other neonatal complications including UAC Solid organ transplantation Congenital heart disease Malignancy or bone marrow transplant Recurrent urinary tract infections, haematuria or proteinuria Treatment with drugs known to raise BP Known renal disease or urological malformation Other systemic diseases associated with hypertension (eg. neurofibromatosis, tuberous sclerosis, sickle cell disease etc.) Family history of congenital renal disease Evidence of elevated intracranial pressure Useful Resources: - Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Flynn JT, Kaelber DC, Baker-Smith CM, et al. Pediatrics. 2017;140(3) - Krishnan, RG & Hegde S.
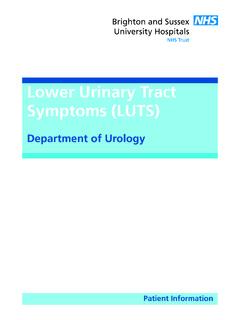
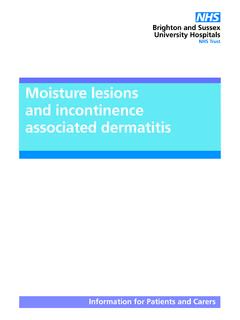
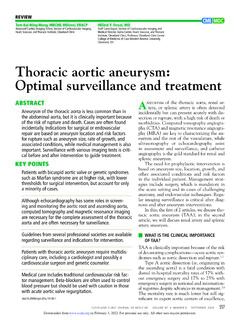
9 Approach to a Hypertensive Child. Welsh Paed J 2009; 30: 6 8. Paediatric Blood pressure tables Appendix 1 Table 1 BP levels for boys by age and height percentile Paediatric Blood pressure tables Appendix 1 cont. Table 1 BP levels for boys by age and height percentile Paediatric Blood pressure tables Appendix 2. Table 2 BP levels for girls by age and height percentile Paediatric Blood pressure tables Appendix 2 cont. Table 2 BP levels for girls by age and height percentile