Transcription of Functional Abilities Form - yyzdistrict301.com
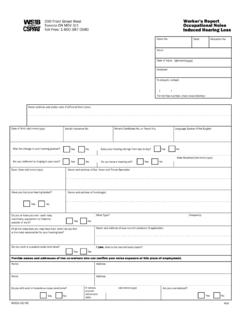
1 FunctionalAbilities form for Planning Early and Safe Return to Work Health Professionals, please use this form ONIY when requested by an employer or worker. The purpose of this form is to identify your patient's overall Functional Abilities and work restrictions that will assist his/her return to suitable work. Your promptness in completing this form is key in assisting the employer and worker to plan an early and safe return to work. Please provide the completed pages 2 and 3. to the worker and/or employer. Authority to Release Information Section37(3) of the WorkplaceSafetyand InsuranceAct,7997 providesthe legalauthorityfor healthprofessionals to givethe WorkplaceSafetyand InsuranceBoard(WSIB), the injuredworkerand the employersuch informationas may be prescribedconcerningthe worker'sfunctionalabilities.
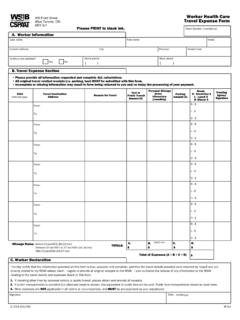
2 Whencompletingthis report,pleaseprint in black ink. Workerand/or employershouldcompleteSectionsA and B of this yourpatientneedsassistance, reportevenif SectionA is not fullycompleted. lnformationaboutyourresponsibilities can be found on Pa$e 4. The WSIB will pay healthprofessionals for completingthis form . Mail to: Fax to: Workpface Safety and lnsurance Board OR 416-344-4684. 200 FrontStreetWest or 1-888-313-7373. Toronto,ON MsV3J1. h FAF. UUSlB Mailto: or Faxto: 200 FrontStreetWest 4L6344-4684. Functional Abilities form d$ffirr- Toronto 0N MsV3Jl 0R 1-888-313-7373. for PlanninglEarly and Safe Return to Work Please PRINT in black ink ClaimNo. A, Section A to be completed by the employer andlol worker. Worker's LastName FirstName Telephone (. (no.,street,apt.). Address City/Town Province PostalCode Employer's Name Dateof Birth (dd/nn/ywy).)
3 (N0,,Street, FullAddress Apt.) DateofAccident/. Awareness of lllness ( ' ). City/Town i;;,. Employer Telephone ,( ). Employer FaxNo. ( ). (where 1. Typeofjobat timeof accident pleaseattachdescription available, ofjobactivities) Area(s). of injury(ies)/illness(es). 2, Havetheworkerand theemployerdiscussed Return ToWork : lf no,willbediscussed on oo mm Ytw t] no contactname 3. Employer Position anyhealthprofessional Bysigningbelow,I amauthorizing whotreatsmeto provideme,myemployer andtheWorkplace Board(WSIB). SafetyandInsurance with information aboutmyfunctionalabilitiesontheWSIB's" Functional Abilities forPlanning EarlyandSafeReturn to Work" form . C, Health Professlonal's Billing tnformation Forbillinspurposesfax or mail pages2 and 3 to the WSIB. INFORMATIONIN SHADEDAREASSHOULDNOTBE PROVIDEDTOTHEWORKEROR EMPLOYER.
4 HealthProfessional's Designation [] CniropractorIl enysician Il Physiotherapistfl RegisteredNurse(ExtendedClass). [ Are you reglstered vesPlease enterthe ninedigitnr$lE ProvfulbilF;=inthe,Sox,provided with theWSlB? I. I call1 - 800 69-?919 to register rcoPlease print). Name(please HealthProfessional's Your lnvoice Numbet I hereby declare that the information being submitted in Sections G, D, E and F of this form is tlue and complete. lt is an offense to knowingly make a fals6 or misleading statement or representation to the WSIB. Telephone ( ): 2647 A (O7/06) paEe2 of 4. Ints*rE200 FrontStreetWest FAF. Mailto: or Faxto: Functional Abilities form 416344-4684 for Planningl Early CSBHTT oronto0N MsV3J1 0R 1-888-313-7373 and Safe Return to Work Please PRINT in black ink Worker's LastName First Name No.]
5 Glaim D, The following information should be completed by the Health Professional to identify the patient's oyerall Abilities and restrictions. 1. Date of dd mm yyry 2. Pleasecheckone: Assessment f PatientiscaDableof Patient of returning iscaDable is physicially Patient unableto L'. 7 returninEtoworkwith toworkwith restriction-s retumto workatthistime. no reslrictions. Complete E and F. sections Complete sectionF. E. Abilities and/or Restrictions indicate 1. Please Abilities detailsin section additional 3. Walking: Standing: Liftingfromfloortowaist: ll Fulabitities Fullabilities Fullabilities Fullabilities ! uptoloometres Upto15 minutes Upto30minutes Upto 5 kilograms - 15 - 30 minutes 5 - 10 kilograms ]too zoometes 30minutes-1hour I I other(pleasespecify) 0ther(please specify) other(pleasespecify) other(please specify).
6 Liftingfromwaistto shoulder: Stairclimbing: Ladder climbing: Travelto work: ' r Fultabilities Fullabilities Fullabilities Abilityto use Abilityto ! unto 5 kitograms Upto 5 steps 1 - 3 steps publictransit drivea car l ]5- l0kilograms 5 - 10steps 4 - 6 steps lves fves l l Other(please specify) Other(please specify) Other(please specify). [.]rvo l]ruo 2. Please indicateRestrictions detailsin section additional 3. : I Limiteduseof hand(s): l B e n d i n g / t w i s t i n g , I w o r k a t o r a b o v e: ! Cnemical fl - Environmental Left Right repetitive movement of shoulderactivity: i exposure to: exposureto: ( , (pleasespecify) : i cold,noiseorscents) tl n [. cripping Pinching 0ther(pleasespecify). F. T. I Limitedpushing/pullingwith: [ motorized Operating equipment: fl Potentialsideeffectsftom i I ExPosuretovibration: ( ) medications (please specify).
7 ! lertarm Donotincludenamesof . fl whotebody ___jRightarm medications. I t] Hand/Arm I other(pleasespecif,). 3. Additional Comments on Abilities and/ot Restrictions. 4. Fromthedateofthisassessment, theabovewillapplyforapproximately: : 5. Haveyoudiscussed returnto work r-zuaysI s-zoays[ 8-14days . withvourpatient? I f] 14*oays [ ves I no 6. Recommendationsfor . startDate dd mm Ytfl f] negutarfull-timehours I Modifiedhours [l Graduatedhours workhoursandstartdate: F. Date of Next Appointment dateof nextappointment Recommended to reviewAbilities and/ot Restrictions. I have provided this completed Functional Abilities form to: I Worker and/ot ! Employer page 3 of 4. lmportant Information To receivebenefits,the workermust applyfor benefitswithinsix monthsof the date of a work-related injuryor illness.
8 Whenfilinga claimfor benefits,the workermust also consentto the disclosure of functionalabilitiesinformation providedby a healthprofessional to his or her employerfor the purposeof facilitatingan earlyand safe returnto work. Failureto file a claimor provideconsentfor the releaseof the functionalabilitiesinformationcan resultin no benefits. lf you havequestionsaboutthe completionof this form pleasecall 1-800-387-0750. Worker's Responsibilities . Thisform is to be completedby a treatinghealthprofessional,who will discussthe informationwith you.. Oncecompleted,contactyouremployerimmedia tely to reviewthe informationon the , you and youremployerwill beginto plan an earlyand safe returnto work. Employer's Responsibi lities . Thisform providesgeneralinformationaboutthis worker'sfunctionalabilitiesand restrictions to helpyou planan earlyand safe returnto work.
9 Whenyou providethis form to the treatinghealthprofessional, ensurethat you havethe worker'ssignedconsent (SectionB)for the releaseof functionalabilitiesinformation.. Whereavailable,also attacha descriptionof the worker'sjob activitiesto assistthe healthprofessional in completing the form .. The prescribed form that is availablefrom the WSIBis a genericform developedto assistwith generalfunctionalabilities information.. TheWSIB will paythe healthprofessional to completethe prescribed WSIB form chargewill appearon your AccidentCoststatementor Schedule2 Invoicewhichreflectsthe costof paymentfor eachform completed.. lf you havea form that is specificto yourworkplaceand havethe cooperation of the workerin providingconsentfor the releaseof informationon yourform,you may use yourown form . lf you createyourown form ,you must reimbursethe healthprofessional directly.
10 Do not senda copyof the completedFunctional AbilitiesFormfor PlanningEarlyand Safe Returnto Workto the WSIB. The healthorofessional is resoonsible for submissionof the form . Health Professional's Responsibilities . Theemployerand workerwill use this informationto planthe worker'searlyand safe returnto work.. Theirreturn to work planswill reflectthe functionalabilitiesand restrictions you havenotedand presumethat no clinical contraindications existfor otherwork activities, thereforeit is crucialthat all sectionsbe completedin full.. Thecompletionof this form is basedon yourexamination of the workerand doesnot requirea specialized functiona abilitiees valuation.. Diagnostic or confidentialinformationmust not be included.. Pleaseadd specificinformationon the durationof temporaryrestrictions or maximumtimes or weightsto be considered, in sectionE3 underabilities and/ot restrictions.