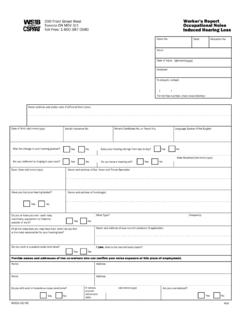
Transcription of Worker Health Care Travel Expense Form
1 Toronto Ottawa London Windsor Kitchener Kingston St. Catharines Northhome print Hamilton Bay Thunder Bay Sudbury Timmins Guelph Sault Ste. Marie Print Home 200 Front Street Worker Health Care West Toronto ON print reset Print Reset Travel Expense Form M5V 3J1. Please PRINT in black ink. Claim Number (mandatory). A. Worker Information reset resetReset this Reset This page Page Last name First name Initial Current address City reset this ResetProvince This Postal Code page Page Is this a new address? Home phone Work phone Yes No ( ) ( ). B. Travel Expense Section Please provide all information requested and complete ALL calculations. All original Travel related receipts ( parking, taxi) MUST be submitted with this form. Incomplete or missing information may result in form being returned to you and/or delay the processing of your payment. Personal Mileage Meals Taxi or (kms) Treating Date Travel Destination Parking B - Breakfast $. Reason for Travel Public Transit kilometers Agency (mm/dd/yyyy) Address Amount ($) L - Lunch $ Signature Amount ($) (roundtrip) D- Dinner $.
2 B-$. From: L-$. Please print form & sign before returning to the WSIB. To: D-$. From: B-$. L-$. To: D-$. From: B-$. L-$. To: D-$. From: B-$. L-$. To: D-$. From: B-$. L-$. To: D-$. From: B-$. L-$. To: D-$. B-$. From: L-$. To: D-$. A. B. (rate X km) C. D. Mileage Rates: Before 01 Jan2001 ($ ) TOTALS: Between 01 Jan2001 to 31 Dec2005 ($ ) $ $ $ $. After 01 Jan2006 ($ ). Total of Expenses (A + B + C + D) $. C. Worker Declaration I hereby certify that the information provided on this form is true, accurate and complete, and that the Travel details provided were incurred by myself and are directly related to my WSIB related claim. I agree to provide all original receipts to the WSIB. I also authorize the release of any information to the WSIB. relating to the Travel details and expenses listed on this form. 1. If traveling other than by personal vehicle or public transit, please obtain and provide all receipts. 2. If public transportation is available but alternate mode is chosen, the equivalent of public fare will be paid.
3 Public fare transportation based on local rates. help/tips 3. Meal expenses are NOT applicable in all claims or circumstances, and MUST be pre-approved by your adjudicator. Help/Tip Signature Date: mm/dd/yyyy home Please print form & sign before returning to the WSIB Home 2721A (04/06) print WTEF. Print