Transcription of Modified Treadmill Protocol for Evaluation of …
1 1 ActaPHYSIOLOGICA&PHARMACOLOGICAB ulgaricaResearch articleModified Treadmill Protocol for Evaluation of PhysicalFitness in Pediatric Age Group - Comparison with Bruceand Balke ProtocolsB. Marinov1, S. Kostianev1, T. Turnovska2, 1 Department ofPathophysiology and 2 Department of Hygiene & Ecology, HigherMedical Institute, Plovdiv, aim of this study was to compare classical Balke and Bruce protocols with our modification of Balkeprotocol in pediatric cardiorespiratory diagnostics. The modification of Balke consists of nine stages per 1 minat a constant velocity of and increasing elevation from 6% to 22% in 2% healthy children (mean age= years; BMI= ; mean 95% CI), divided intothree groups of 20 children each, matched by age, height and BMI performed integrative cardiopulmonaryexercise testing using one of the Treadmill protocols mentioned.
2 At the end of each exercise increment andthroughout the recovery period the children were asked to rate the perceived exertion (RPE) using the BorgCategory Ratio scale - results showed that Balke Protocol had the longest duration ( min.) and the lowest valuesfor VO2/kg ( ) due to the minimal workload increments. Bruce Protocol had intermediateduration ( min.) and children achieved the highest VO2/kg ( ) but the test issymptom-limited which is ethically unacceptable in childhood. Exercise data revealed that our modificationof the classical Balke Protocol had an optimal duration (11 min.)
3 And yielded peak VO2/kg values( ) adequate for Evaluation of children s exercise capacity. Children s ratings of perceivedexertion were highest in Bruce Protocol ( ) and lowest in the original Balke Protocol ( ).In conclusion, the modification of Balke Protocol is suitable and reliable for screening and clinical testingin pediatric age Physiol. Pharmacol. Bulg., 27 (2003) WORDS: Treadmill protocols; Exercise tolerance in children; Perceived exertion; Borg February 21, 2002 INTRODUCTIONC ardiopulmonary exercise testing not only mea-sures the efficiency and capacity of the oxygen trans-port systems but can also reveal the causes for children sexercise limitation (Armstrong and Welsman, 1994).
4 Historically, the protocols used for exercise testinghave been based on tradition, convenience or the past decade a considerable amount of researchhas focused on the effect of the exercise Protocol ontest performance, including exercise tolerance, diag-nostic accuracy and gas exchange (Myers et al.,2000). Children s performance largely depends on theexercise modality and the testing Protocol (Washing-ton et al., 1994), though special considerations haveto be taken to tailor the workload to pediatric popu-lation and ensure standard conditions.
5 There areseveral widely used Treadmill protocols for assess-ment of children s physical capacity but none of themis compliant with the modern guidelines for paediat-ric exercise testing (Washington et al., 1994). There-fore there is a necessity of a Treadmill Protocol ap-propriate either for a clinical use or as a reliablescreening method. Such Protocol is intended to avoidboth an excessive duration and excessive workloadincrements (Myers et al., 1991; Buchfuhrer et al.,1983). Since pediatric patients are of various ages andsizes, sometimes disabled with respect to mobility andmuscular coordination the new Protocol must bedesigned to change either speed or grade from onestage to the next (Lehman et al.)
6 , 1997)The aim of this study was to compare classicalBruce and Balke Treadmill protocols with our modi-Corresponding author: Blagoi Marinov, MD, 15A Vasil AprilovBlvd, Higher Medical Institute, Pathophysiology Department,Plovdiv 4002, Bulgaria. Phone: (+359 32) 602227;e-mail: Physiologica et Pharmacologica Bulgarica2fication of Balke Protocol in pediatric population, aswell as to elucidate the applicability of the new pro-tocol in AND METHODSS ixty healthy children (mean age years),divided into three groups of 20 children each, matchedby age, height and BMI (Table 1) performed integra-tive cardiopulmonary exercise testing using one of thefollowing Treadmill protocols.
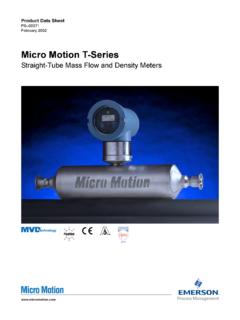
7 Balke Protocol (Balke and Ware, 1959) con-stant velocity of mph ( km/h) and 1%increments each minute till 22%. Bruce Protocol (Bruce, 1971) simultaneouslychanging speed and grade in 3 minutes intervals. Modified Balke Protocol (Marinov et al., 2000) consisting of nine stages per 1 min at a con-stant velocity of km/h and increasing eleva-tion from 6% to 22% in 2% increments presentation of the three applied pro-tocols is shown on Fig. of the children were in good health, physi-cally active but not engaged in a regular endurancetraining activities.
8 Prior to the test all the participantsunderwent comprehensive pulmonary function as-sessment: conventional spirometric tests (slow vitalcapacity and forced vital capacity) and maximal in-spiratory pressure (PImax) with MasterScreen Diffu-sion (Jaeger, Wuerzburg, Germany) in a certifiedlaboratory applying the ERS (Statement, 1993) andATS (Statement, 1995) criteria to ensure quality. Allmeasurements were performed in a seated positionwith a nose clip. Thorough anthropometric measure-ments were performed as Treadmill test was performed in the morningin a laboratory compliant with the modern guidelines(Pina et al.)
9 , 1995). The children were habituated toboth the general environment and the actual testprocedures. The exercise test was carried out on amotor driven, electronically controlled Treadmill (TrackMaster , USA) and gas exchange variableswere determined with an on-line computerized sys-tem CardiO2 (Medical Graphics, MN, USA) usingstandard open circuit techniques. Subjects breathedthrough a mouthpiece and a pneumotachometer wasused for recording tidal volume (VT; , BTPS)and minute ventilation (VE; , BTPS). Expiredgas samples were analyzed for oxygen and carbondioxide by zirconium oxide and infrared analyzers,respectively.
10 Data were averaged every 30 sec andwere used to calculate oxygen uptake (VO2), carbondioxide production (VCO2) and respiratory exchangeFig. 1. Graphical presentation of the applied Treadmill 27 (2003) pp-pp3ratio (RER). The system was calibrated before eachtest. Heart rate was monitored electrocardiographi-cally (Hellige, Germany).At the end of each exercise increment and through-out the recovery period the children were asked torate the perceived exertion (RPE) using the BorgCategory Ratio scale - CR-10 (Borg, 1982) depictingfatigue (dyspnea) from not at all to maximal bymeans of ten in anthropometrical and peak exercisevariables were assessed with regard to the groupsstudied and different protocols using descriptive sta-tistics of SPSS for Windows (SPSS, Chicago, IL,USA).