Transcription of Protocol: Water Deprivation Test - Walter Reed Bethesda
1 1 protocol : Water Deprivation TestApproved by the Scientific Advisory Committeeof the Diabetes Insipidus Foundation, Robertson, , Committee Chair*Heinz Valtin, , CoordinatorPreambleThis document is directed primarily to physicians who may wish to conduct a waterdeprivation test on their own. The reader will soon sense that a complete, properlyperformed test is a complicated procedure that requires specially trained , we recommend that when a Water Deprivation test is needed , when thepatient's basal plasma sodium concentration is within the normal range while the concurrenturine osmolality is below 300 mOsm/kg H2O the patient be referred to a , for those physicians who prefer to run the test on their own, an abbreviated testcomprising only Phase I ( , Steps 1 through 6 under Procedure) may suffice to diagnoseeither complete (severe) neurogenic or complete (severe) nephrogenic DI.
2 We stress thateven an abbreviated Water Deprivation test must be started in the morning and must beconducted in a controlled setting where the patient is observed constantly throughout theentire , however, the patient concentrates the urine in response to fluid Deprivation before theplasma sodium concentration rises out of the normal range [ , if Step (b) under Procedure 5occurs before Step (a)], then Phase II (Step 7) will be required in order to make the difficultdifferential diagnosis among primary polydipsia, partial neurogenic DI, and partialnephrogenic DI. Inasmuch as Step 7 entails the measurement of plasma vasopressin (AVP)concentration (which is performed with the required accuracy in only a few selectlaboratories), and often entails as well the monitored infusion of hypertonic saline, Phase IIshould be performed only in specialized of TestTo distinguish among the major forms of Diabetes Insipidus (DI):(a) neurogenic (or central or pituitary), where the Water diuresis results from a deficiency ofthe antidiuretic hormone, arginine vasopressin (AVP);(b) nephrogenic, where the Water diuresis results from an inability of the kidneys to respondto AVP.
3 (c) polydipsic (also known as primary polydipsia), where the Water diuresis results from thesuppression of AVP release by excessive fluid modified version of the test may be used to verify2(d) gestagenic, where the Water diuresis results from destruction of AVP by the placentalenzyme, of the measurement of plasma osmolality is widely available, relatively fewlaboratories carry out this measurement with the degree of accuracy required for the waterdeprivation test (see Potential Problems and Pitfalls). Plasma sodium concentration cansubstitute for plasma osmolality in this test, and the sodium concentration is measured withthe required accuracy in virtually all laboratories. We therefore advise the substitution ofplasma sodium for plasma osmolality in most instances. (These cautionary notes do notapply to the measurement of urine osmolality .)
4 Furthermore, both osmolality and AVP concentration must be determined on plasmaobtained from heparinized blood rather than on serum or plasma obtained from EDTA-treated blood. Throughout this protocol , we will specify "plasma sodium concentration"since then all three measurements osmolality , AVP concentration, and sodiumconcentration can be obtained from the same heparinized blood Water Deprivation test should be performed only if the patient's basal plasma sodiumconcentration is within the normal range (and while the concurrent urine osmolality is below300 mOsm/kg H2O) during ad libitum fluid and food basal plasma sodium concentration is above normal while the urine osmolality isbelow 300 mOsm/kg H2O, the Water Deprivation test is unnecessary and potentiallyharmful. In this case, skip to the dDAVP challenge test (see below, under Procedure,Phase I, Step 6).
5 Not perform the Water Deprivation test in patients with: (a) renal insufficiency; (b)uncontrolled diabetes mellitus; (c) hypovolemia of any cause; or (d) uncorrected deficiencyof adrenal or thyroid the test is in progress, carefully monitor Water balance of the patient throughhourly determinations of body weight and plasma sodium concentration (and plasmaosmolality where that varible can be measured with the required accuracy). Dehydrationmay develop rapidly if the patient has severe neurogenic or nephrogenic the patient for the entire duration of the test, not only to prevent surreptitiousdrinking but also to be certain that the results are not confused by non-osmotic stimulants ofAVP secretion , smoking, postural hypotension, vaso-vagal reactions, or other episodesof nausea or I Abbreviated Form: through Step 6 but not the test between 7 and 9 am, and have someone with the patient throughout the patient should not eat or use tobacco for at least 2 hours before and during the continued drinking ad libitum while completing the following five preparations inthe order given.
6 (i) place patient recumbent for 30 minutes, during which steps ii - v can becarried out (patient may sit or stand during voiding of urine and determinationof weight)(ii) insert and firmly anchor a heparin lock in an arm vein(iii) collect 7 - 10 ml of heparinized blood into an iced tube and send it to the labfor immediate processing (results available within 20 to 30 minutes) andmeasurement of sodium concentration (and osmolality if it can be measuredaccurately). Freeze 2 ml of plasma for later assay of AVP(iv) ask patient to empty her/his bladder, record the urine volume, and send thesample to lab for stat measurement of osmolality . Patient may stand briefly tovoid(v) weigh patient to nearest kg and record the value as well as the bloodpressure and complete fluid restriction and keep patient in semi-recumbent position, except forshort periods of standing if that is necessary to void hour, repeat steps iii, iv, and v above, and record patient's symptoms, if there these steps until one of the following occurs.
7 (a) plasma sodium concentration or osmolality rise above upper limit of normalor(b) urine osmolality rises above 300 mOsm/kg H2 OSubsequent steps will vary depending on which event occurs (a) OCCURS BEFORE (b), then primary polydipsia, partial neurogenic,and partial nephrogenic DI are excluded, and a challenge test with dDAVP (desamino-d-arginine vasopressin, also called desmopressin) should be done to determine whetherthe patient has complete (severe) neurogenic or complete (severe) nephrogenic Challenge 2 micrograms ( g or mcg) of dDAVP patient to empty bladder at 1 and 2 hours after the injection and measurethe osmolality of these either sample has an osmolality more than 50% higher than the valueimmediately before dDAVP was given, the patient probably has complete(severe) neurogenic the rise in urine osmolality after dDAVP is less than 50%, then complete(severe) nephrogenic DI is very likelyPhase II Requires Trained Personnel and Specialized (b) IN STEP 5 OCCURS BEFORE (a), complete (severe) neurogenicand complete (severe) nephrogenic DI are excluded, and the procedures outlined inStep 6 cannot be used to further differentiate among partial nephrogenic DI, partialneurogenic DI, and primary polydipsia.
8 In this situation, several other approachesshould be preferred method is to measure plasma AVP on samples collected before and duringwater Deprivation (Steps 2, 3, and 4 under Procedure) and interpret the results in relationto the concurrent plasma sodium concentration (or plasma osmolality , if sufficientlyaccurate) as well as against the concurrent urine osmolality (Figs. 1 and 2). [NOTE:Interpretation of the results is always clear when plasma sodium and plasma osmolalityare above the normal range. If this does not occur through Water Deprivation alone,infuse hypertonic (3%) saline at ml per kg body weight per minute and measureplasma sodium (and osmolality if sufficiently accurate) stat every 30 minutes until theyrise above the normal range; measure plasma AVP concentration in the same samples.]
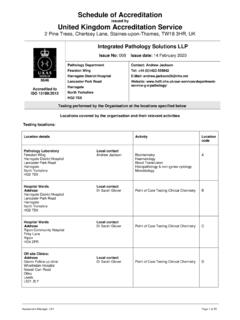
9 ]These results can be interpreted as follows: If under basal conditions, plasma AVP is higher than 2 pg/ml, while duringfluid Deprivation it is normal or high in relation to the concurrent plasmaosmolality (Fig. 1b) or plasma sodium concentrtion (Fig. 2) -- and falls to theright of the normal (shaded) area in relation to the urine osmolality (Fig. 1a) --the patient has partial nephrogenic DI If under basal conditions, plasma AVP is less than 1 pg/ml, while during fluiddeprivation and/or hypertonic saline infusion it is below normal in relation tothe concurrent plasma osmolality (Fig. 1b) or plasma sodium concentration(Fig. 2) -- and is normal or lower than normal in relation to the urineosmolality (Fig. 1a) the patient has partial neurogenic DI If under basal conditions, plasma AVP is less than 1 pg/ml, while during fluiddeprivation and/or hypertonic saline infusion it is normal in relation to theconcurrent plasma osmolality (Fig.)
10 1b) or plasma sodium concentration ( ) and falls within the normal (shaded) area in relation to the urineosmolality (Fig. 1a) the patient has primary Sodium (mEq/L)120130140150160 Plasma Vasopressin (pg/mL )051015 LDNormalRangeNephrogenic DINeurogenic DIPrimary polydipsic DIFigure 1. Results of the Water Deprivation test on normal subjects (shaded areas) and patientswith the three major forms of diabetes insipidus. Each plotted symbol represents asimultaneous sampling for two variables: plasma AVP (the antidiuretic hormone, argininevasopressin) and urine osmolality (Fig. 1a); and plasma osmolality and plasma AVP ( ). The interrupted lines denote the limit of the assay for plasma AVP; below the limitingvalue, no AVP can be detected in the plasma. The data come from patients seen by Dr. GaryL.