Transcription of Saving Lives, Improving Mothers’ Care
1 Maternal, Newborn and Infant Clinical Outcome Review Programme Saving Lives, Improving Mothers' Care Core report : lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017-19. November 2021. Maternal, Newborn and Infant Clinical Outcome Review Programme Saving Lives, Improving Mothers' Care Core report : lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017-19. Full report available at Marian Knight, Kathryn Bunch, Derek Tuffnell, Roshni Patel, Judy Shakespeare, Rohit Kotnis, Sara Kenyon, Jennifer J Kurinczuk (Eds.). November 2021 . Funding The Maternal, Newborn and Infant Clinical Outcome Review Programme, delivered by MBRRACE-UK, is commis- sioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the National Clinical Audit and Patient Outcomes Programme (NCAPOP).
2 HQIP is led by a consortium of the Academy of Medical Royal Colleges, the Royal College of Nursing, and National Voices. Its aim is to promote quality improvement in patient outcomes. The Clinical Outcome Review Programmes, which encompass confidential enquiries, are designed to help assess the quality of healthcare, and stimulate improvement in safety and effectiveness by systematically enabling clinicians, managers, and policy makers to learn from adverse events and other relevant data. HQIP holds the contract to commission, manage, and develop the National Clinical Audit and Patient Outcomes Programme (NCAPOP), comprising around 40 projects covering care provided to people with a wide range of medical, surgical and mental health conditions.
3 The Maternal, Newborn and Infant Clinical Outcome Review Programme is funded by NHS England, NHS Wales, the Health and Social Care division of the Scottish government, The Northern Ireland Department of Health, and the States of Jersey, Guernsey, and the Isle of Man Design by: Sarah Chamberlain and Andy Kirk Cover Artist: Tana West Printed by: BCQ. This report should be cited as: Knight M, Bunch K, Tuffnell D, Patel R, Shakespeare J, Kotnis R, Kenyon S, Kurinczuk JJ (Eds.) on behalf of MBRRACE-UK. Saving Lives, Improving Mothers' Care - CORE report lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017-19.
4 Oxford: National Perinatal Epidemiology Unit, University of Oxford 2021. ISBN: 978-1-8383678-7-9. 2021 Healthcare Quality Improvement Partnership and National Perinatal Epidemiology Unit, University of Oxford MBRRACE-UK - Saving Lives, Improving Mothers' Care 2021 - Core report Foreword As we write this foreword, the Birthrights inquiry into Racial Injustice in Maternity Care is analysing evidence from hundreds of Black, Brown and mixed ethnicity women and birthing people about their experiences and the impacts of systemic racism on their care. Emerging themes, backed up by testimony from healthcare professionals, include feeling unsafe, their concerns being ignored or dismissed, denial of pain relief due to racial stereotypes, and perva- sive microaggressions causing harm or distress.
5 This MBRRACE-UK report shows yet again the stark disparity in maternal mortality rates between women from Black and Asian aggregated ethnic groups and White women more than four times higher for Black women, two times higher for mixed ethnicity women and almost twice as high for Asian women. Apart from a slight drop in the maternal mortality rate for Black women, this bleak picture has not changed in over a decade. We remain deeply concerned that Black and Brown people's basic human rights to safety, dignity, respect and equal- ity in pregnancy and childbirth are not being protected, respected or upheld. Our inquiry has also heard how previous life experiences racist attitudes, microaggressions, dismissal of concerns, breakdown of trust can affect interactions with maternity services.
6 This report cannot capture the impact of this prior experience, but it must be recognised and better understood. Although we cannot hear the voices of the women whose deaths are examined in this MBRRACE-UK Confiden- tial Enquiry, it is clear that basic human rights are still challenged at many levels. Women do not receive essential contraceptive and pre- pregnancy advice because of structural and cultural biases. The fact of women's pregnancy still leads to investigations such as x-rays, as well as essential medications, being withheld because of a culture focusing entirely on potential risk, rather than benefit. Gaps in postnatal care are stark. It is also very evident how other factors socioeconomic deprivation, language difficulties, mental health problems, obesity, domestic abuse combine to increase the impact of the structural and cultural biases women experience simply because they are, have been, or might become, pregnant.
7 Birthrights began our inquiry recognising that systemic racism exists in society as a whole so it must also impact maternity care. We must also understand the systemic, multi-layered discrimination against pregnant women and birthing people which prevents them receiving the best care before, during and after pregnancy and which may result in the ultimate tragedy of a maternal death. These facts are not new and action is long overdue. We must all play a part in the solution whether through advocacy, recognising the impacts of our own bias, validat- ing a mother's experiences and concerns, or simply being the one person to listen and act. Sandra Igwe Amy Gibbs Co-Chair Chief Executive Inquiry on Racial Injustice Birthrights in Maternity Care MBRRACE-UK - Saving Lives, Improving Mothers' Care 2021 - Core report i Key messages from the report 2021.
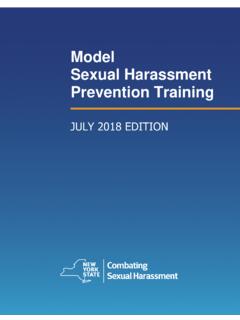
8 In 2017-19, 191 women died during or up to six weeks after the end of pregnancy , from causes associated with their pregnancy , among 2,173,810 women giving birth in the UK. women per 100,000 died during pregnancy or up to six weeks after childbirth or the end of pregnancy . There is no statistically significant difference in maternal mortality compared to 2010-12. Preventing maternal deaths - we are all part of the solution ay become pregna om nt, w h are en Train Train pr e om g undergraduates postgraduates w na at Advocate nt Tre ,o Remember Counsel rw the benefits post- pregnancy of Work ho treatment Individualise as a multidisciplinary . pathways of care h a ve son not to team Advise pre- pregnancy Recognise recently be including on contraception the Provide abnormal postnatal r re a care Remember risk is Offer a Give safety specialist mental e dynamic en net advice Avoid gaps and physical yc l health in care or p Reassess services treatment r r eg e Prevent risk v obesity n a Remember self a is n examination tt re Understand Stop h e t he and gate sa tackle keeping 4x ss me l e inequity n u as a no n-pregnant person ii MBRRACE-UK - Saving Lives, Improving Mothers' Care 2021 - Core report Executive Summary Introduction This report .
9 The eighth MBRRACE-UK annual report of the Confidential Enquiry into Maternal Deaths and Morbidity, includes surveillance data on women who died during or up to one year after pregnancy between 2017 and 2019 in the UK. In addition, it also includes Confidential Enquiries into the care of women who died between 2017 and 2019. in the UK and Ireland from mental health-related causes, venous thromboembolism, homicide and malignancy. The report also includes a Morbidity Confidential Enquiry into the care of women who gave birth aged over 45 years. Surveillance information is included for 495 women who died during or up to one year after the end of pregnancy between 2017 and 2019.
10 The care of 37 women who gave birth aged over 45 years was reviewed in depth for the Confidential Enquiry chapter. This report can be read as a single document; each chapter is also designed to be read as a standalone report as, although the whole report is relevant to maternity staff, service providers and policy-makers, there are specific clini- cians and service providers for whom only single chapters are pertinent. There are seven different chapters which may be read independently, the topics covered are: 1. Surveillance of maternal deaths 2. Older maternal age (morbid- ity enquiry) 3. Mental health and multiple adversity 4. Malignancy 5. Venous thromboembolism. Methods Maternal deaths are reported to MBRRACE-UK, NIMACH or to MDE Ireland by the staff caring for the women concerned, or through other sources including coroners, procurators fiscal and media reports.