Example: stock market
TEST REQUEST FORM
Last 4 Digits of SSN MRN # (will display on report) E-mail (optional) Physician Last Name, First Name Physician Street Address City, State, Zip Code OfÞ ce/Physician Phone # Physician/Authorized Signature Date TEST REQUEST FORM RETURN THIS FORM TO LITHOLINK WITH YOUR COMPLETED URINE SAMPLES LLK0001 (Rev. 10/2017)
Information
Domain:
Source:
Link to this page:
Documents from same domain

CONVERSION TABLE
d2xk4h2me8pjt2.cloudfront.netBilirubin, Direct umol/L x 0.058 = mg/dL Bilirubin, Paediatric umol/L x 0.058 = mg/dL Bilirubin, Total umol/L x 0.058 = mg/dL Bilirubin, Unconjugated umol/L x 0.058 = mg/dL C-Peptide pmol/L x 0.003 = ng/mL C-Reactive Protein (CRP) mg/dL x …

Laboratory Test Tube Color Guide Common lab tests sorted ...
d2xk4h2me8pjt2.cloudfront.netLipase Green – invert 4-5 times to ensure proper mixing of additives Lipid Panel Includes: Trig, Chol, HDL, Calc LDL degrees, then returning it Green – invert 4-5 times to ensure proper mixing of additives Lithium Gold – invert 4-5 times to ensure proper mixing of additives
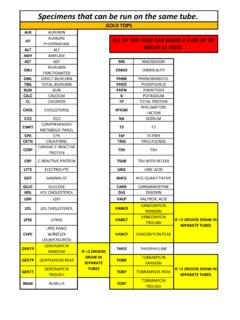
Specimens that can be run on the same tube.
d2xk4h2me8pjt2.cloudfront.netbrain natriuretic peptide green tops gold tops. mono mono test preg pregnancy pregr pregnancy w/reflex hcg msls measles igg bchc hcg tumor marker crl cryptococcal antigen lac lactic acid ghgb glycohgb (hba1c) cbc heme profile (complete blood count) cbca heme profile (complete blood count)w/auto diff rbcf red cell folate esr sed rate
Related documents

MATHEMATICS (IX-X) (CODE NO. 041) Session 2021-22
cbseacademic.nic.in4. Rationalization (with precise meaning) of real numbers of the type and (and their combinations) where x and y are natural number and a and b are integers. 5. Recall of laws of exponents with integral powers. Rational exponents with positive real bases (to be done by particular cases, allowing learner to arrive at the general laws.)

MIPS Assembly Language Guide
www.cs.uni.edulw $4, 16($3) $4 [Mem at address in $3 + 16] sw $4, Mem Mem $4 Memory Access lw $4, Mem $4 [Mem] (Load and Store) Register Transfer Language Description MIPS Assembly Language Type of Instruction Common MIPS Instructions (and psuedo-instructions) A simple MIPS assembly language program to sum the elements in an array A is given below:.data

The accuracy of measurements of viscosity of liquids
nvlpubs.nist.govpapers [4,5]. 2. Systematic Errors in Absolute Measurements Nearly all absolute measurements of viscosity have been based on capillary fl ow because of the high precision attainable. The analysis of capillary measure ments is based on the Poiseuille equation, (1) where Pz is the pressure gradient along the capillary