Transcription of ACNRMJ10:Layout 1 23/4/10 05:25 Page 32 PAEDIATRIC ...
1 Introduction and definitionsThis article provides a systematic approach to thecauses of developmental delay and the impor-tance of its rigorous investigation. It particularlyhighlights practical aspects relevant to adult neu-rological development most commonly followsthe usual pattern of development where skills areacquired more slowly ( Down s syndrome).Less commonly, skill acquisition can be disor-dered ( autism). Delay is a misnomer chil-dren with developmental problems rarely catchup , and will usually have continuing difficultieswith learning later in delay is common, affecting 1-3% of the delay isdefined as significant delay (more than two stan-dard deviations below the mean) in one or moreof the following developmental domains:2mGross motormVision & Fine motormHearing, Speech & LanguagemSocial, Emotional & BehaviouralDevelopmental delay is a descriptive term used forchildren whose difficulties are apparent earlier inchildhood where a cause is not yet established.
2 Itdoes not imply a particular organic or syndromiccause, and the term does not appear in focus of this article is Global Developmental Delay. Causes of Global Developmental DelayGlobal developmental delay can be the present-ing feature of a huge number of neurodevelop-mental disorders (from learning disability to neu-romuscular disorders). It is not possible to pro-vide an exhaustive list; Table 1 gives an approachto evaluation and investigation can reveala cause in 50-70% of ,1 This leaves a largeminority where the cause is not determined. It isstill useful to investigate globally delayed devel-opment whatever the age of the child (occasion-ally older children with significant disability maynot have been investigated adequately).
3 Developmental Delay Causes and InvestigationAngharad V Walters is a Specialist Registrar in PAEDIATRIC Neurology atAddenbrooke s Hospital,Cambridge. She studiedPhysiology and Medicine atBristol University. She is trainingin PAEDIATRIC Neurodisability andhas a particular interest in learning disability and behaviour. Correspondence to:Email: NEUROLOGYTABLE 1: Causes of global developmental delay (adapted from Forsyth and Newton 20075).CategoryCommentsGenetic or Syndromic Easily identified syndromes Down s syndromeIdentified in ~ 20% of those without Genetic causes that are less obvious in early childhood Fragile X, Velo-cardio-facial syndromeneurological signs, dysmorphic features (22q11 deletion), Angelman s, Soto s, Rett's, maternal Phenylketonuria, Mucopolysaccharidoses,or a family historyDuchenne Muscular Dystrophy, Tuberous Sclerosis, Neurofibromatosis Type 1, and subtelomeric deletionsMetabolic Nationwide universal neonatal screening for Phenylketonuria (PKU) and Medium-chain acyl-Co A Identified in ~1% of those withoutDehydrogenase deficiency (MCAD).
4 Neurological signs, dysmorphic features Urea Cycle a family historyEndocrine There is universal neonatal screening for congenital hypothyroidismTraumatic Acquired brain injuryEnvironmental Causes Children require their basic needs for food, clothes, warmth, love and stimulation to be met to develop normally. Children in neglectful, abusive, fearful, under stimulated environments may not show normal development. This can be a contributory factor co-existing with other pathology and where the child s needs are outside the parents capacity to provide for Malformations Neuronal Migration DisordersCerebral Palsy and Developmental Motor difficulties can prejudice development in generalCoordination Disorder (Dyspraxia)Infections Perinatal Rubella, CMV, HIV Neonatal meningitisToxins Fetal: Maternal alcohol or drugs in pregnancy Childhood: Lead toxicityDevelopmental Delay can be dividedinto.
5 Global developmental delay delay in two or more domains (often delayed in all domains)Specific developmental delay ( Motor or Speech & Language) delay in a single domain32>ACNR>VOLUME 10 NUMBER 2 >MAY/JUNE 2010 ACNRMJ10:Layout 1 23/4/10 05:25 Page 32 ACNR>VOLUME 10 NUMBER 2 >MAY/JUNE 2010>33 Why is finding a cause important?Establishing a cause has many benefits for thechild and family and improves overall qualityof life:4mThe family gains understanding of the condition, including prognostic informationmLessens parental blamemAmeliorates or prevents co-morbidity byidentifying factors likely to cause secondary disability that are potentially preventable surveillance of other systems such asvision and hearingmAppropriate genetic counselling aboutrecurrence risk for future children and thewider familymAccessing more support ( within education services and specific syndrome support groups)
6 MTo address concerns about possible events during pregnancy or delivery1mPotential treatment for a few conditionsInvestigation of Global DevelopmentalDelayThorough history and examination are vital toproduce a formulation of the child s problemand target investigations ,6 Thediagnosis may occasionally be immediatelyobvious from history and examination. Moreoften time is needed to review clinical fea-tures, case notes, prior investigations and toconsult the literature, dysmorphology and neu-rogenetic of a patient into your clinic frompaediatric services is a good opportunity toreview the diagnostic process.
7 Most investiga-tions are likely to have been performed earlyin the child s life; medical advances especiallyin genetic investigations and neuroimagingtechniques may allow further diagnostic possi-bilities now. Clinical geneticists are an invalu-able source of diagnostic acumen and sugges-tions for further suitable evidence base for investigation of devel-opmental delay is poor and published work ismainly consensus There is no oneagreed recipe for the investigation of globaldevelopmental delay and there is much varia-tion in practice. Historically, there has beenpatchy introduction of tests as they becameavailable.
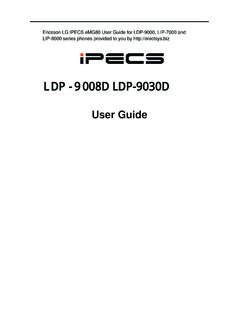
8 This means it is well worth reviewingwhat investigations have actually been scheme illustrating the investigations con-sidered for global developmental delay isshown in Figure 1. You should expect the firstline investigations to have been done, and rel-evant second line investigations depending onclinical : The approach to performing investigations isinfluenced by:midentifying treatable conditionsmidentifying prevalent serious conditions( Creatinine Kinase for DuchenneMuscular Dystrophy)meconomic considerations (inexpensive,easy to perform tests for less common disorders, Fragile X)mthe practicalities of performing the investigations on young childrenPAEDIATRIC NEUROLOGYF irst LineChromosomesFragile XU & ECreatinine KinaseThyroid FunctionFBCF erritin Vision and Hearing assessmentsMetabolicFamily Histor yConsanguinityRegressionOrganomegalyCoar se FeaturesSeizuresAbnormal Head SizeEpisodic decompensationCongenital AtaxiaSensory impairment Including Glue EarBloodLactate (+/- CSF Lactate)
9 AmmoniaAmino AcidsLeadVLCFAAcyl CarnitinesBiotinidaseHomocysteineTransfe rrinsWC enzymes7-DehydrocholesterolUrineOrganic AcidsGAGsOligosaccharidesMRICT for bones, calcificationConsider24hr EEGC onsiderTelomeresMicroarraysMyotonic DystrophyAngelman sPrader-WilliMECP2 NeuroimagingAbnormal Head SizeSeizuresNeurological signsCranial nerve abnormalitiesCerebral palsyNeurocutaneous signsDysmorphic facies ArthrogryposisSevere visual impairmentOptic atrophyNystagmusEEGS eizuresSpeech RegressionGeneticsDysmorphismAbnormal GrowthSensory ImpairmentUnusual BehavioursFamily HistorySecond LineFigure 1: A scheme illustrating the investigationsconsidered for global developmental delay (adapted fromMcDonald et al 20062and A guide to investigation ofchildren with developmental delay in East Anglia 2005 ) 1 Notes: MECP2 = gene for Rett s VLCFA = Very Long Chain Fatty Acids are forPeroxisomal disorders ( Adrenoleukodystrophy) GAGs = Glycosaminoglycans are forMucopolysaccharidoses ( MPS type III Sanfilippo) WC enzymes = White cell enzymes.
10 These andoligosaccharides are tests for lysosomal storagedisorders ( GM1 Gangliosidosis). Transferrins are for congenital disorders ofglycosylation (CDG) type 1a 7-dehydrocholesterol is for Smith-Lemli-Opitz Paired CSF and plasma lactate are to investigatemitochondrial disorders where there are concernsabout growth, multisystem involvement, visual andhearing impairments, and abnormal MRI :Layout 1 23/4/10 05:25 Page 3334>ACNR>VOLUME 10 NUMBER 2 >MAY/JUNE 2010 PAEDIATRIC NEUROLOGYS imple blood tests can be achievedwithout too much brain may require a general anaes-thetic. This may have been delayed if thechild was approaching an age (~ 5yrs ordevelopmental equivalent) where theycould manage an MRI without an anaes-thetic.