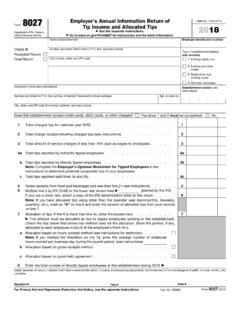
Transcription of Form 712 Life Insurance Statement OMB No. 1545-0022
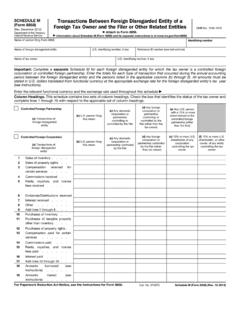
1 INSTRUCTIONS TO PRINTERSFORM 712, PAGE 1 of 4 MARGINS: TOP 13mm (1 2 ), CENTER : HEAD to HEADPAPER: WHITE WRITING, SUB. 20. INK: BLACKFLAT SIZE: 432mm (17") x 279mm (11") FOLD TO: 216mm (81 2") x 279mm (11")PERFORATE: ON THE FOLD712 FormOMB No. 1545-0022 (Rev. April 2006)Life Insurance StatementDepartment of the TreasuryInternal Revenue ServiceDecedent Insured (To be filed by the executor with Form 706, United States Estate (and Generation-Skipping Transfer) Tax Return, orForm 706-NA, United States Estate (and Generation-Skipping Transfer) Tax Return, Estate of nonresident not a citizen of the United States.)Decedent s social security number(if known)Date of deathDecedent s last name432 Decedent s first name and middle initial1 Name and address of Insurance company5 Policy numberType of policy76 Date assignedAssignor s name.
2 Attach copy issued111098 Owner s name. If decedent is not owner,attach copy of of beneficiariesAmount of premium (see instructions)Value of the policy at thetime of assignment141312$Face amount of policy15$Indemnity benefits16$Additional insurance17$Other benefits18$Principal of any indebtedness to the company that is deductible in determining net proceeds19$Interest on indebtedness (line 19) accrued to date of death20$Amount of accumulated dividends21$Amount of post-mortem dividends22$Amount of returned premium23$Amount of proceeds if payable in one sum24$Value of proceeds as of date of death (if not payable in one sum)25 Policy provisions concerning deferred payments or If other than lump-sum settlement is authorized for a surviving spouse, attach a copy ofthe Insurance policy.
3 $Amount of installments27 Date of birth, sex, and name of any person the duration of whose life may measure the number of applied by the Insurance company as a single premium representing the purchase ofinstallment benefits29$Basis (mortality table and rate of interest) used by insurer in valuing installment sWas the insured the annuitant or beneficiary of any annuity contract issued by the company?3335 Names of companies with which decedent carried other policies and amount of such policies if this information is disclosed by your undersigned officer of the above-named Insurance company (or appropriate federal agency or retirement system official) hereby certifies that this Statement setsforth true and correct of Certification Title Signature Form712(Rev.)
4 4-2006)Cat. No. 10170 VPart SPECIFICATIONSTO BE REMOVED BEFORE PRINTINGDO NOT PRINT DO NOT PRINT DO NOT PRINT DO NOT PRINTTLS, have youtransmitted all Rtext files for thiscycle update?DateActionRevised to printWere there any transfers of the policy within the three years prior to the death of the decedent?Date of assignment or transfer://Month Day YearDid the decedent have any incidents of ownership on any policies on his/her life, but not owned byhim/her at the date of death?313234 NoYe sNoYe s15161718192021222324252729 For Paperwork Reduction Act Notice, see page 712 (Rev. 4-2006)Living Insured(File with Form 709, United States Gift (and Generation-Skipping Transfer) Tax Return.
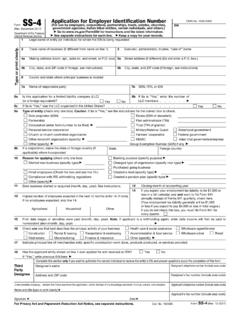
5 May also be filed with Form 706, UnitedStates Estate (and Generation-Skipping Transfer) Tax Return, or Form 706-NA, United States Estate (and Generation-SkippingTransfer) Tax Return, Estate of nonresident not a citizen of the United States, where decedent owned Insurance on life of another.)SECTION A General InformationSocial security numberLast nameFirst name and middle initial of donor (or decedent)383736 Date of gift for which valuation data submitted 39 Date of decedent s death for which valuation data submitted 40 SECTION B Policy Information41 Date of birth43 Sex42 Name of insured44 Name and address of Insurance company45 Issue date48 Face amount47 Policy number46 Type of policy49 Frequency of payment50 Gross premium51 Date assigned52 Assignee s name53 Datedesignated56 Date of birth,if known55 Sex54If irrevocable designation of beneficiary made, name ofbeneficiary57If other than simple designation, quote in full.
6 Attach additional sheets if policy is not paid up:58 Interpolated terminal reserve on date of death, assignment, or irrevocabledesignation of beneficiaryaAdd proportion of gross premium paid beyond date of death, assignment,or irrevocable designation of beneficiarybAdd adjustment on account of dividends to credit of policycTotal. Add lines 58a, b, and indebtedness against policyeNet total value of the policy (for gift or estate tax purposes). Subtract line 58e from line 58dfIf policy is either paid up or a single premium:59 Total cost, on date of death, assignment, or irrevocable designation ofbeneficiary, of a single-premium policy on life of insured at attained age, fororiginal face amount plus any additional paid-up Insurance (additional faceamount $)a(If a single-premium policy for the total face amount would not have beenissued on the life of the insured as of the date specified, nevertheless, assumethat such a policy could then have been purchased by the insured and statethe cost thereof, using for such purpose the same formula and basis employed,on the date specified, by the company in calculating single premiums.)
7 Adjustment on account of dividends to credit of policybTotal. Add lines 59a and 59bcOutstanding indebtedness against policydNet total value of policy (for gift or estate tax purposes). Subtract line 59d from line 59ceThe undersigned officer of the above-named Insurance company (or appropriate federal agency or retirement system official) hereby certifies that this Statement setsforth true and correct ofCertification Title Signature INSTRUCTIONS TO PRINTERSFORM 712, PAGE 2 of 4 MARGINS: TOP 13mm (1 2 ), CENTER : HEAD to HEADPAPER: WHITE WRITING, SUB. 20. INK: BLACKFLAT SIZE: 432mm (17") x 279mm (11") FOLD TO: 216mm (81 2") x 279mm (11")PERFORATE: ON THE FOLDPart SPECIFICATIONSTO BE REMOVED BEFORE PRINTINGDO NOT PRINT DO NOT PRINT DO NOT PRINT DO NOT PRINT58a58b58c59a59b59c59d59e58f58d58eFo rm712(Rev.)
8 4-2006)INSTRUCTIONS TO PRINTERSFORM 712, PAGE 3 of 4 (PAGE 4 IS BLANK)MARGINS: TOP 13mm (1 2 ), CENTER : HEAD to HEADPAPER: WHITE WRITING, SUB. 20. INK: BLACKFLAT SIZE: 432mm (17") x 279mm (11") FOLD TO: 216mm (81 2") x 279mm (11")PERFORATE: ON THE FOLDI nstructionsPaperwork Reduction Act Notice. We ask for theinformation on this form to carry out the InternalRevenue laws of the United States. You are required togive us the information. We need it to ensure that youare complying with these laws and to allow us to figureand collect the right amount of of insurer. This Statement must be made,on behalf of the Insurance company that issued thepolicy, by an officer of the company having access tothe records of the time needed to complete and file this form willvary depending on individual statements.
9 File a separate Form 712 foreach 13. Report on line 13 the annual premium, not thecumulative premium to date of you have comments concerning the accuracy ofthese time estimates or suggestions for making thisform simpler, we would be happy to hear from are not required to provide the informationrequested on a form that is subject to the PaperworkReduction Act unless the form displays a valid OMBcontrol 712 (Rev. 4-2006) SPECIFICATIONSTO BE REMOVED BEFORE PRINTINGDO NOT PRINT DO NOT PRINT DO NOT PRINT DO NOT PRINTP rinted on recycled paperFor purposes of this Statement , a facsimile signaturemay be used in lieu of a manual signature and if used,shall be binding as a manual death occurred after the end of the premiumperiod, report the last annual or records relating to a form or its instructionsmust be retained as long as their contents maybecome material in the administration of any InternalRevenue , tax returns and return information areconfidential, as required by section the instructions for the tax return with which thisform is filed.
10 Do not send the tax form to that , return it to the executor or representative whorequested estimated average time is:Recordkeeping 18 hrs., 11 about the form 6 the form 23 min.