NEW yorkpaidFamilyLeave (PFL)BOND with a childCARE for a Family memberASSIST military familiesPaid FamilyLeave may also be available for use in situations when you or your minor dependent child are under an order of quarantine or isolation due to COVID-19. See for full for 202167% Wage BenefitsReceive 67% of your average weekly wage, up to a to 12 Weeks of LeaveCan be taken all at once, or in full-day Protections Return to same or comparable job. Continued health insurance. No discrimination or Can Request PFL?Generally, Employees Who: Work for a private employer in new york state , or a public employer who has opted in. Meet the time-worked requirements: Full-time (regularly work 20 or more hours/week), after 26 consecutive weeks of employment. Part-time (regularly work fewer than 20 hours/week), after 175 working to Request PFLGive 30 days notice to your employer, if request forms and submit to your employer s insurance pays or denies benefits within 18 days of receiving your completed the website for more information and to download PFL request the toll-free PFL Helpline 8:30 to 4:30 , FAMILIES, STRONG NEW YORKPFL-ov-graphic-2021-v1 9-20
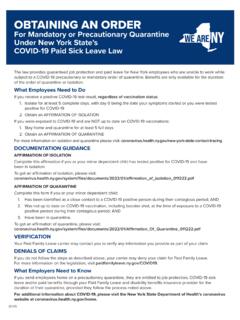
New York State, or a public employer who has opted in. Meet the time-worked requirements: • Full-time (regularly work 20 or more hours/week), after 26 consecutive weeks of employment. • Part-time (regularly work fewer than 20 hours/week), after 175 working days. How to Request PFL Give 30 days’ notice to your employer, if foreseeable.
Transcription of New York Paid Family Leave at-a-glance fact sheet
1 NEW yorkpaidFamilyLeave (PFL)BOND with a childCARE for a Family memberASSIST military familiesPaid FamilyLeave may also be available for use in situations when you or your minor dependent child are under an order of quarantine or isolation due to COVID-19. See for full for 202167% Wage BenefitsReceive 67% of your average weekly wage, up to a to 12 Weeks of LeaveCan be taken all at once, or in full-day Protections Return to same or comparable job. Continued health insurance. No discrimination or Can Request PFL?Generally, Employees Who: Work for a private employer in new york state , or a public employer who has opted in. Meet the time-worked requirements: Full-time (regularly work 20 or more hours/week), after 26 consecutive weeks of employment. Part-time (regularly work fewer than 20 hours/week), after 175 working to Request PFLGive 30 days notice to your employer, if request forms and submit to your employer s insurance pays or denies benefits within 18 days of receiving your completed the website for more information and to download PFL request the toll-free PFL Helpline 8:30 to 4:30 , FAMILIES, STRONG NEW YORKPFL-ov-graphic-2021-v1 9-20
Complaints about employer discrimination or retaliation are resolved by a Workers’ Compensation Board Law Judge after a hearing. If you believe that your employer has discriminated or retaliated against you for taking or requesting Paid Family Leave, visit PaidFamilyLeave.ny.gov or contact (844) 337-6303.
STATEMENT OF RIGHTS If you need to take time off from work to care for a family member, you may be entitled to paid family leave benefits ... Employees with a regular work schedule of less than 20 hours per week are eligible after 175 days worked. Citizenship or immigration status is not a factor in your eligibility.
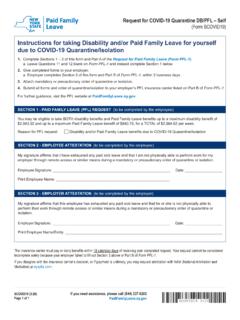
Attach mandatory or precautionary order of quarantine or isolation. 4. ... If you disagree with the insurance carrier’s decision, or if payment is untimely, you may request arbitration with NAM (National Arbitration and . Mediation) at nyspfla.com. PART A - EMPLOYEE INFORMATION (to be completed by the employee)
SECTION 1 - PAID FAMILY LEAVE (PFL) REQUEST (to be completed by the employee) Reason for PFL request: Care for minor dependent child subject to COVID-19 Quarantine/Isolation. 1. Minor dependent child’s name (first name, middle initial, last name) 2. Minor child’s date of birth (MM/DD/YYYY) 3. Minor child’s mailing address. Street address
“Employers” section of PaidFamilyLeave.ny.gov. · Collect employee payroll contributions to pay for the insurance. You may withhold employee contributions at the rate set by DFS each year to pay for the cost of the insurance until employees reach their annual maximum contributions.
Leave should continue to collect employee contribution during periods of paid time off. Model language: Time spent on paid vacation, sick or personal days can be counted toward an . employee’s eligibility determination. Time out on short-term disability does not count towards an employee's eligibility determination. 3.
Based on your average pay period earnings of $ _____. _____, your estimated pay period deduction will be: $ _____. _____. Note: This deduction may fluctuate pay period to pay period, depending on your hours worked. For more information, visit PaidFamilyLeave.ny.gov or call the Paid Family Leave Helpline for assistance at (844) 337-6303.
Based on your average pay period earnings of $ _____. _____, your estimated pay period deduction will be: $ _____. _____. Note: This deduction may fluctuate pay period to pay period, depending on your hours worked. For more information, visit . PaidFamilyLeave.ny.gov. or call the Paid Family Leave Helpline for assistance at(844) 337-6303.
Mail or fax your Form PFL-1 and Form PFL-4 to your employer’s insurance carrier. To find out who your employer’s insurance carrier is, you can: Look for the Paid Family Leave poster in your workplace. Ask your employer. Use the employer coverage search application on wcb.ny.gov to …
The New York State Workers’ Compensation Board protects the rights of employees and employers by ensuring the proper delivery of benefits and by promoting compliance with the law. To learn more about the Board, visit wcb.ny.gov. QUESTIONS The Workers’ Compensation Board (Board) can help you understand your Schedule Loss of Use claim.
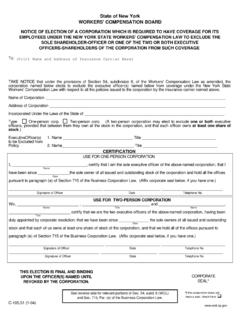
state of new york workers' compensation board notice of election of a corporation which is required to have coverage for its employees under the new york state workers' compensation law to exclude the sole shareholder-officer or one of the two or both executive officers-shareholders of the corporation from such coverage
Prescribed by Chair, Workers' Compensation Board. STATE OF NEW YORK - WORKERS' COMPENSATION BOARD. CHECK ONE. Address Claimant. Attorney or Representative Insurer. Employer* NOTICE TO ATTORNEY OR REPRESENTATIVE: 1. This form may be used by an . original, substituted or additional. attorney or representative. Check appropriate box on top of …
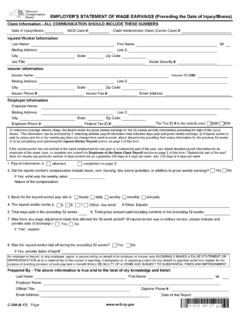
2. Did the injured worker's compensation include board, rent, housing, tips and/or gratuities, in addition to gross weekly earnings? If Yes, what was the weekly value: Nature of the compensation: Yes. No 3. Basis for the injured worker pay rate is: hourly. daily weekly. monthly annually 4. The injured worker works a: 5. 6 7. Other. 5.
pedestrian deaths in the U.S. Five states alone account for 43% of all pedestrian deaths—California, Florida, Texas, New York, and Arizona. The reported number of smartphones in active use in the U.S. rose 236% from 2010 to 2016, said the report, which cited an increase in cell phone-related _ emergency room visits.
7. ADJUSTMENTS TO COMPENSATION. 21 Notwithstanding any other provision of law, no ad-22 justment shall be made under section 601(a) of the Legis-23 lative Reorganization Act of 1946 (2 U.S.C. 4501) (relat-24 ing to cost of living adjustments for Members of Congress) 25 during fiscal year 2021. December 21, 2020 (10:27 a.m.)